One of the most common developmental Problems in children is the
occurrence of intoeing/out-toeing. If you have noticed that your child's feet turn in (or
out), this condition is often considered normal and, with time, your child's feet will
return to the normal position without the need for treatment.
What Is intoeing/Out-toeing?
Out-toeing usually occurs during the first 12 months due to the hip
positioning while in the uterus. Out-toeing will resolve without any form of treatment.
Intoeing develops from one of three areas: the foot, the knee, or at the
hip.
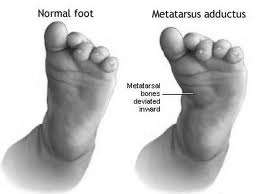
The Foot: Metatarsus Adductus
This is the most common cause of intoeing from birth to 2 years of age
and is believed to be caused by positioning in the uterus, or family history. If the foot
is flexible and can be gently pulled into the correct position, no treatment is necessary.
If the foot is rigid and your child is under 8 months of age, your physician may recommend
casting.
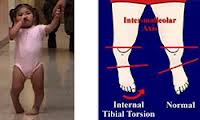
The Knee: Tibial Torsion
This is noticed most commonly during the second year of life after the
child has started walking. The shin bone (tibia) is slightly twisted or rotated causing
the foot to turn in. This may be due to the position while in the uterus, a family history
or may even be aggravated by the child sitting on his/her feet.
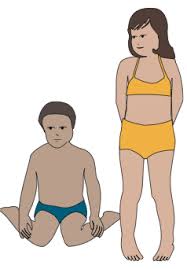
The Hip: Fernoral Anteversion
Children between the ages Of 3 and 7 may walk with their knee caps
pointing inward This is caused by a slight rotation of the top of the hip bone (femur) in
the socket of the hip. Usually this occurs more often in
girls, and may be aggravated by sitting in the "W" position
What Is the Treatment for Intoeing/Out-toeing? Observation is the best treatment for out-toeing and intoeing. You can take
pictures of your child standing, at yearly intervals, and then compare the progression of
the straightening process.
Very rarely is another form of treatment necessary. Only if, for some
reason, your child does not "growout of this condition" by the age of 10 will
surgical options be considered.
1 . Your child's intoeing is a common developmental condition.
2. BRACING, TWISTER CABLES, AND CORRECTIVE SHOES
ARE NOT NECESSARY. Many years ago, it was believed that these
treatments helped correct intoeing, but years of studies have shown them NOT to be
effective.
3. Falling is a part of the learning to walk process and is not
exclusively caused by intoeing.
4. Sitting "Indian style" is better than having your child sit
on his/her feet or in the "W" position.
5. Intoeing will not affect your child's abilities to walk, run, play,
or lead a normal life.
We have been sleeping babies on their backs for many
years now and the incidence of crib death has dramatically decreased. But
we also stopped most pigeon toed… toeing in. When we slept the kids on the
stomach their feet were curled in and under as in this picture.

This twisted their lower leg Tibia bone in ward and
bent the front half of the foot inward. The terms for these are Tibia
Torsion and Metatarsus Adductus. These conditions had to be treated and we
had to put them in a splints as shown.
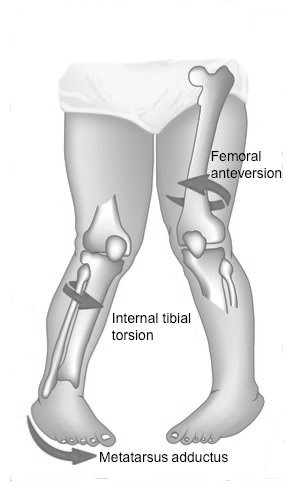


You can tell if it is Tibial Torsion from another
condition that is Femoral Antiversion because the outside ankle bone is in
front of the inside ankle bone.
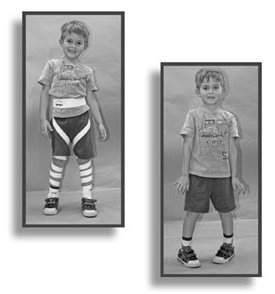
The kids tend to sit on the floor legs outward with
Femoral Antiversion. Encourage them to sit cross legged. We don’t treat
the Femoral antiversion but they used to put them in this contraption to
make it look better. They will generally grow out of it and these devises
did not make a difference.
We almost never have to treat these conditions since
the mild forms will go away through the years of running and playing. We
hardly ever see severe forms since we sleep them on their backs.
So sleep them on their backs.....

Roger Knapp MD
