Nov 2, 2009
We are in this area seeing a decline in cases of Swine Flu.
I was seeing 20-30 cases a day and now it is 3-4 a day.
The cases are on the upswing in other areas of America.
The deaths are continuing and mainly because there is such a
huge number of cases.
The number of deaths are not as many as 2008 regular flu cases.
Hopefully we will get the flu vaccine in ... supposed to be
here any day... supposed to have been here
weeks ago.
Dr. Knapp
Oct 26, 2009
There is a massive number of cases of Swine flu. It is
just now moving more up North. We actually are over the hump here and
are seeing a
decline in cases. There now have been roughly 4 times as many cases of
Swine flu as there are regular seasonal flu cases in the winter.
In the 2007-2008 season there were 80 deaths in children and 80 % of
them had major health problems.
The President announcing this as a National Emergency was a
move designed to expedite disaster plans should hospitals get overwhelmed.
There are approximately 4 times as many cases of swine flu, then we should
see 320 deaths but there have been less.
There were 67 deaths last winter from the regular flu. There were 45
deaths from last Spring to Oct 09 from Swine flu.
There were 53 deaths since Oct 1 which is the beginning of the 2009-2010
season. That is a total of 98 deaths ... instead of 320.
Remember the children who should get Tamiflu should have
major health issues.... it is not just for everyone with the flu.
Also remember any fever after three days of flu cough and fever, we need to
give them antibiotics for secondary pneumonia.
You can see how these cases and deaths stack up but not
bad... see See:
http://www.cdc.gov/flu/weekly/
We do not have H1N1 swine flu injectable vaccine and will
post info at the flu clinic area when we do or sign up for Newsymail
and we will be sending out info.
Dr. Knapp
Oct 9, 2009
The news now has the report of the children dieing of the
flu. There are 2-3 times more cases of flu this year as apposed to
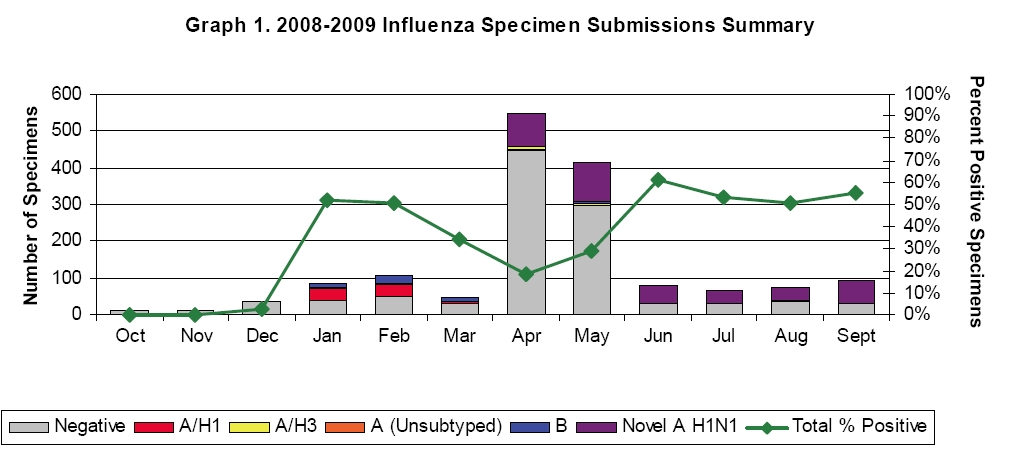
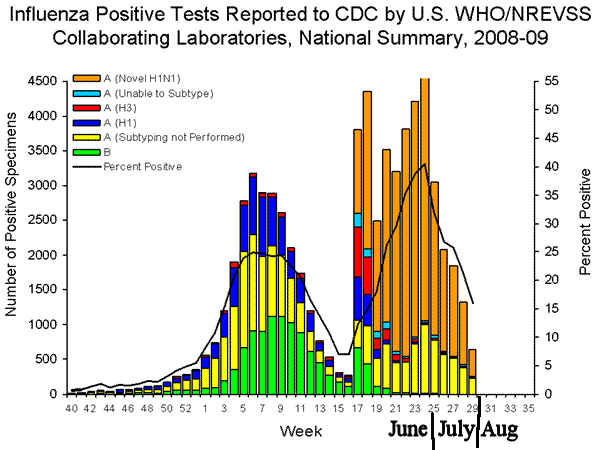
previous years. See this graph from the CDC:
The first hump of cases to week 16 is our normal cases of
flu. As you can see there are many more cases
from week 16 to week 39. There is normally only a very few cases or
none after week 16.
So with more cases then there
will be more deaths ... tragically. So if we look at this year's deaths
to this week:
You can see there are more illnesses in the Spring, Summer and Fall
when we normally do not see any.
So if there are 2-3 times increase in flu cases, then the deaths should be twice or
more increase over
the normal number. That means 2 times 80 would give 160 to 240 cases.
But there has only been
76 tragic deaths from the H1N1 flu. This new flu is just as
dangerous as the old flu but there are
fewer deaths.
There are children and adults that die every
year of the flu... the news media
usually does not mentioned them on the evening
news. That is why we have
a vaccine for Chicken Pox. There were a few children who died of
chicken pox every year and
you were never aware of them. It was infrequent, tragic, but happened.
I think we are over the peak of the cases of swine flu and should be on
the down slope of cases (just when we
are about to get the vaccine!). But then we will have the regular flu
starting in December.
Dr. Knapp
p.s. History note: The Boy Scouts were to have their first National
Jamboree in 1935. Weeks before the event
they cancelled it even though preparations, tickets, posters and everything
was all ready for the event.
They cancelled it because of the big outbreak of Polio that year and they
did not want to spread it
with all the boys coming from all over America to one spot. The first
Jamboree was finally held in 1937.
Parents who are against all vaccinations like meningitis, polio, and other illnesses are idiots.
Oct 8, 2009 Well the CDC came out with recommendations
for the new H1N1 vaccine that will be soon delivered.
They recommend that patients that had confirmed Swine H1N1
illness (that was documented by Reverse Transcriptase testing by the CDC
which almost no one's virus was tested) do not have to receive the vaccine.
All others should get the vaccine .... even those that had tested positive
for Type A flu by rapid testing in the doctor's office. The test has
many false negative tests and some false positive (meaning you don't have
type A flu but test came out positive anyway.)
The number of false positives is very low. And the
Type A flu since last May have been 99.6 % H1N1 swine flu. But because
of the rare false positive, they want every one of those patients to get the
shot just to be sure. The illness stimulates very good immunity to
this flu. The regular seasonal flu will be coming in Dec-March and
then it will be impossible to know if the illness is regular flu or swine
flu if the test is pos for type A flu.
My personal opinion:
1. If you had a rapid test positive for Flu A then it was very likely
you had the H1N1 swine flu. I don't think you need the vaccine but it
will not hurt you to get one if you so desire.
2. If you had a negative test (which misses around 50% of the cases)
but had "classic" symptoms, you probably do not need the vaccine but again
it will not hurt you to get it if you so desire and want to be 100% sure.
3. If you had a classic case of illness with 2-3 days of fever and
were not tested for the flu, then you probably do not need the vaccine but
again it will not hurt you to get the vaccine if you so desire.
4. If you had a mild illness and really not classic flu symptoms, or
did not get ill this Fall, then get the vaccine. (which is safe... see
below.)
Dr. Knapp
Oct 7, 2009
This was an email I answered yesterday about the safety:
This is probably a question you are getting from so
many, but what do you
really think about the H1N1 vaccine? I'm sure you've seen or heard
about the doctor on one of the news stations that's posted on youtube
saying that he thinks the vaccine is more dangerous than swine flu itself.
That is crazy. There was a problem with
swine flu vaccine in the 1970s
With a illness Guillian Barre. The difference was so small in
comparison
to the general population It occurs in normal people at
1/100,000.
The vaccine in 1970s increased the chances so slightly that it then
was 1 in a million chance of the vaccine causing this in patients.
But 36,000 adults and 100 kids die every year from the flu. Far
better
to get the vaccine.
SEE:
http://www.cdc.gov/h1n1flu/vaccination/gbs_qa.htm
What are the mercury levels like in the swine flu vaccine and
the regular flu vaccine? My 3 girls already got their shots at your
office for seasonal flu. Do you think there are risks with doing both?
Is the swine flu higher in mercury or any other preservatives that
might be dangerous than other vaccinations?
The vaccines are safe. The mercury does not cause health issues
like
Autism. The amount of mercury is so miniscule that you get more
mercury
in the fish you eat. And it is the Methyl mercury that hurts you
from the fish.
The Ethyl mercury in vaccines clears out of your body quickly. They
Have to put something in the vaccines to keep it sterile... either
mercury or formaldehyde.
But It is not enough to cause you any problems.
See:
http://www.myomancy.com/2005/05/ethyl_mercury_v
And, are you encouraging your grandchildren to be vaccinated against
H1N1?
Most definitely they will get it.
Dr. Knapp
Opinion Sept 5, 2009
There are a lot more cases of flu this year which we
expected since no one is immune to this.
Many of the case deaths are from bacteria and
especially pneumonia after day 3. So if your child has typical symptoms of
flu (fever, headache, sore throat, mild cough, and pain in the windpipe with
cough, and body aches) there is usually 3 days of fever, day 4 has fever of
100 and better, and day 5 has 99 fever and feels better still. Any high
fever 101 or more after day three, see the doctor or fill out the
prescription of antibiotic that I gave you. The children who have died of
the flu are frequently kids with pneumonia after day 3. That is what the 14
yr old who died of the flu in Fort Worth this last weekend. She had fever
Wed and Thur and Fri. She saw the doctor Friday and he appropriately did
not give Tamiflu. But she started with high fever and lethargy day 4 on Sat
and did not get care until Sunday. So watch for fever after day three of
the flu. Tamiflu is for the high-risk kids; it only shortens fever one day;
does not stop the shedding of the virus; and does not reduce the chances of
secondary infections very much. You still have to watch out for pneumonia.
See:
http://www.cdc.gov/mmwr/preview/mmwrhtml/mm58e0929a1.htm?s_cid=rr58e0929a1_e
There is not an increase in deaths from the flu and
pneumonia :
See:
http://www.cdc.gov/flu/weekly/
As you can see
from these graphs, there are more visits with flu now but less mortality.
Hard to say why. Maybe all the kids who were susceptible to dieing have
already been exposed? But there are more cases now. The top graphs show
the increase and WOW what a difference. I have never seen this in the
30 yrs of practice. This new strain is sweeping the world. It is
not more dangerous but there are a lot more cases. And if you look at
the middle graph above of deaths from flu and pneumonia, there is not an
extreme increase. The news again has you scared. So watch for the fever
after day 3 and get antibiotics quickly if that occurs. That has been true
even years ago with the regular flu. There have been deaths but the
news did not broadcast it and you were not aware of them.
We do not know when we will get
the swine flu vaccine in our office. The news says we will get the
nasal flu first but high risk cannot get that one. So it looks like we
will give the first vaccine to the low risk kids first. ???? duh!.
The high risk groups will be getting the shot when it comes in. I
think most kids will have gotten this new flu before we give the vaccine.
I think it will be recommended for the high risk group first but it will be
given to those who are in our office and ask for it. So it will
probably be first come first serve. We are expected to get enough
vaccine to give every one a vaccine for the swine flu. But we will not
have enough of the regular flu vaccine for the regular flu that comes in
this winter. Don't rush to get the regular flu vaccine since it does
not show up until Dec thru March. Hopefully will give both flu
vaccines to your child at the same time in Nov. We can give both but we
cannot give both nasal live vaccines at the same time. We can give
both injectable or one nasal and one injectable at the same visit. We
still do not know how many vaccines it will take. Adults build up
immunity with just one shot. We will see about the kids and ongoing studies
are measuring it right now.
Dr. Knapp
Oct 1, 2009
There is a big shortage all over America of the regular flu
vaccine. We have sadly had to cancel clinics. More vaccine will
come later probably in November. See the article:
http://www.google.com/hostednews/ap/article/ALeqM5jFXWlf10vStMfubD5l6VhQ1PxNGAD9B2H50O2
This is a great explanation of the shortage.
When we get the swine flu vaccine sometime this month
(hopefully... ) and more of it in Nov. there is a recommendation to give it to high risk
patients first.
So it looks like everyone will eventually get both vaccines
but it may be last minute in Nov and Dec.
Dr. Knapp
(and we want government health care???? Yeow!)
Opinion Sept 27, 2009
Well another message about
H1N1 swine flu. We are continuing to be directed by the CDC to only treat
high risk patients and not every one.
We had a patient who had
the swine flu and had a high risk person in the family. By the time we
diagnose the case, the high risk person (adult) was already exposed. You
are most contagious the day before fever. And the medication Tamiflu does
not stop the virus. Studies showed that patients secrete the virus for up
to 10-12 days with or without treatment. The Tamiflu stops the symptoms
sooner. Some studies show less bacterial complications and some studies
show no decrease in them with treatment. So the adult in this case who is
already exposed to the virus needs to consider Tamiflu and we did not treat
the child who was doing well with the illness.
SEE:
http://www.usatoday.com/news/health/2009-09-14-H1N1-swine-flu_N.htm
The liquid medication of
Tamiflu can be confusing. It is 12mg/ml. The eye dropper measures the
medication in MG and not ml (volume). So read the directions carefully.
Also the liquid is almost impossible to find. I have been giving the pills
and have them made into a liquid by the pharmacy or crush them up into food.
SEE:
http://www.webmd.com/cold-and-flu/news/20090925/tamiflu-for-kids-confusing-dosage-can-harm
There is a huge increase of
Swine flu. I am seeing 20+ cases a day. I am not testing many of them
since if it looks exactly like it, because the test does not help since the
test misses half of the cases. Whether it is pos or neg ... it is still
H1N1. Many physicians also do that. So many cases are not reported. We
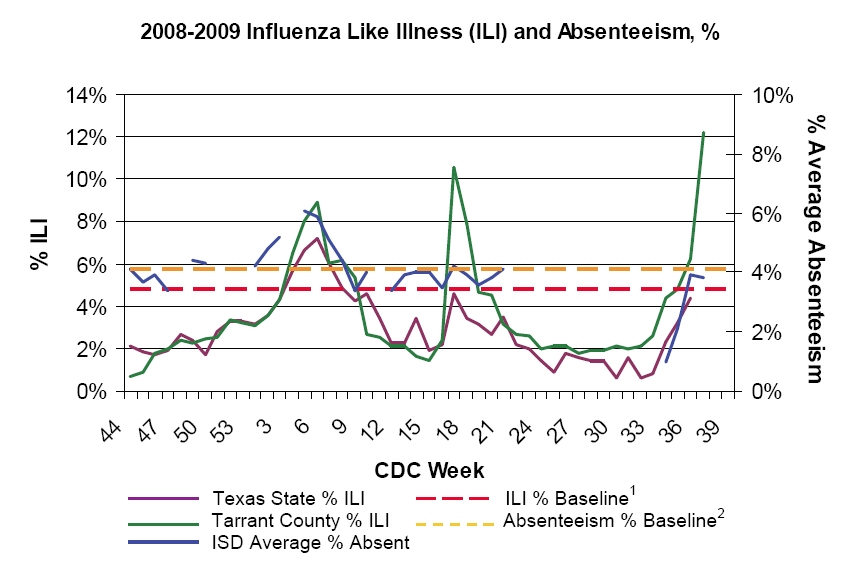
classify them as ILI (influenza like illness). See these two graphs as an
example. First one is the reported cases but the second one is absentees
from ILI. Big increase. Many schools have 100s of kids out. There are far
more cases (not more deadly) than the news will report.
I bet by the time they have
the H1N1 Swine flu vaccine (sometime in Oct), then at that time more than
half of the kids will have already had it. The Government told the drug
companies to produce more swine flu than regular seasonal flu. So there is
now a shortage and we are fast running out of flu shots and have limited
nasal flumist. (Get yours as soon as you can) And by the time we have the
swine flu vaccine in full swine, that type of flu will be on the down slope
and the regular flu will be on the increase in Jan with less people
immunized against it. Remember the two flus are just as dangerous to the
high risk patients. The government is going to be out of sink on their
timing of vaccines in my personal opinion... maybe I'm wrong but we shall
see.
The virus is on most store
cart handles, church pews, restaurants, and other public areas. So
sterilize your hands frequently. Not as many adults are getting sick since
they wash their hands better and do not put their hands in their mouth as
much.
Dr. K
Opinion Sept 16, 2009:
I am now seeing 10 cases of swine flu a day. Most are
not very sick. I am sure the news will come out and say how many thousands
of kids are getting the flu. Closing the schools last Spring just delayed
the spread to now. The CDC finally came out and said to only treat the high
risk patients with Tamiflu. I have preached that for years. If we treat
everyone with Tamiflu then the germ will become resistant. There have been
already a handful of resistant H1N1. If it becomes resistant like the old
flu did, then we will not have anything to help the kids with cancer or the
pregnant moms. So most likely we will not be treating your child. Also the
flu test misses 50%. So if they act like the flu we will approach the child
as if they have it without testing. If the test is pos then they have the
flu, and if neg then they probably still have the flu and the test does not
change what we do. We hope to have the swine flu vaccine by late
Oct. Please come in if you are in the high risk group (See below for list) .
For more info.... see:
http://www.cdc.gov/h1n1flu/antiviral.htm
http://www.dallascounty.org/department/hhservices/documents/DCHHS_Flu_Report_2009_2010_Week_35_Final.pdf
this has great graphs on the big increase in flu in this area and see how
rare in these months of the year.
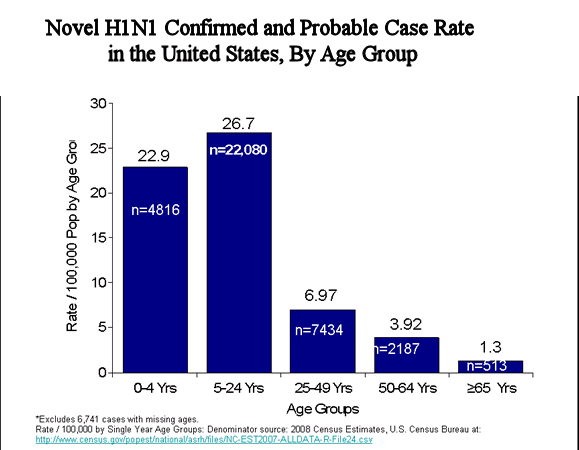
Here is the CDC chart of deaths in children and you
can see there is an increase number because of the increase number of cases…
not because it is more deadly. This is the deaths out of 80 million
children so still very rare.

This graph shows the cases last Spring (in pink).
Just wait till you see the graph that includes this Fall.
The death of the 11yr old girl that died this week was
caused by a mean bacteria and she did not die of the flu itself. Watch for
secondary bacterial infections. Any fever past the 5th day would
be a signal and come in right away.
Roger Knapp MD
Sept 12, 2009
Again news and personal opinion
The vaccine for the H1N1 flu(swine) is close to
production. We will have it late Oct or Nov. Studies show good antibodies
after one shot and they may only recommend one shot instead of 2 shots like
they were suggesting last month. That makes sense to me. You need two
vaccines 1 month apart if it is the first year you get flu vaccines. We
will not know how much vaccine supplies we will have and what age or
category will be given the vaccine. Maybe we will be given enough vaccine
to vaccinate everyone. We shall let you know.
Many parents have asked should I give the H1N1 vaccine
to my child? It is recommended for all children to 18 yrs old. Remember
this flu is not more dangerous than past flu. There will be more cases
because no one is immune to it. My recommendation: do this year what you
usually do. If you think it is a good idea to vaccinate your children to
flu and you have been doing that for years, then vaccinate them to both flu
viruses. If you don’t usually want to vaccinate them in the years past
and you still think it is not for your child, then don’t vaccinate them for
either flu.
Don’t let the news media scare you on this thing. Just
use good hand sanitation all year.
August 09
Personal Opinion. The news is making this out of proportion. It is
a new strain and many people will not be immune to it. So there
will be more cases this year but it is not more dangerous than previous
years. Ignore the news that scares you into watching their
programs. We should not close schools so talk to your school districts
and keep the schools open. People are most contagious
the day before symptoms and can shed virus for 7 days. Most will tell
them to go back to school when no fever for 24 hours.
They already exposed others when coming down with it. Masks will not
prevent you from catching it but ill people should wear
masks so they do not spread it easily. We should not treat all people with Tamiflu and other meds.
They should be treated if in a
high risk group. If your
child had type A flu in May, June, July Aug then you are probably immune to
H1N1 and the vaccine may not be necessary.
Otherwise I do recommend the vaccine for the regular flu and for the swine
H1N1 flu in everyone over 6 months. They will be
separate shots. The swine flu will not be available in the nasal drops
and only in shot form.
36,000 adults die every year from the flu and approx 180 kids die every
year... out of 100s of millions. Most have other health issues.
Very kids will die that are otherwise healthy. 1/million. We
mostly worry about kids <2yr, lung problems, cancer, immune problems,
heart problems, and pregnant mothers. Also the family of small infants <6
months should get shots to avoid them getting it.
July 09
These are some excerpts from CDC
recommendations for Swine H1N1 flu. You will see that the main individuals
who should be treated with flu meds like Tamaflu are those at high risk.
Not everyone with the flu should get it. If everyone is treated, then the
germ will become resistant like last year’s flu virus. If it becomes
resistant through over use, then we do not have medication to help those who
are high risk.
Main CDC site:
http://www.cdc.gov/h1n1flu/
The novel influenza A (H1N1) virus is
susceptible to both neuraminidase inhibitor antiviral medications zanamivir
and oseltamivir. It is resistant to the adamantane antiviral medications,
amantadine and rimantadine. Antiviral treatment with either oseltamivir or
zanamivir is recommended for patients who are hospitalized or who are at
higher risk for seasonal influenza complications. Rare sporadic cases of
oseltamivir resistant novel influenza A (H1N1) viruses have been detected
worldwide. Additional information on antiviral recommendations for treatment
and chemoprophylaxis of novel influenza A (H1N1) infection is available at
http://www.cdc.gov/h1n1flu/recommendations.htm
See video of their
recommendations. http://www.youtube.com/watch?v=L8oyiT-oZ-I
Antiviral Resistance
This novel (H1N1) influenza virus is sensitive (susceptible) to the
neuraminidase inhibitor antiviral medications, zanamivir and oseltamivir. It
is resistant to the adamantane antiviral medications, amantadine and
rimantadine.
Antiviral Treatment for Novel (H1N1)
Influenza
For antiviral treatment of novel influenza (H1N1) virus infection, either
oseltamivir or zanamivir are recommended. Recommendations for use of
antivirals may change as data on antiviral effectiveness, clinical spectrum
of illness, adverse events from antiviral use, and antiviral susceptibility
data become available.
Treatment is recommended for:
All hospitalized patients with confirmed, probable or suspected novel
influenza (H1N1).
Patients who are at higher risk for seasonal influenza complications (see
the following).
High-risk groups:
A person who is at high-risk for complications of novel influenza (H1N1)
virus infection is defined as the same for seasonal influenza at this time.
As more epidemiologic and clinical data become available, these risk groups
might be revised.
- Children younger than 5 years old.
The risk for severe complications from seasonal influenza is highest
among children younger than 2 years old.
- Adults 65 years of age and older.
- Persons with the following
conditions:
Chronic pulmonary (including
asthma), cardiovascular (except hypertension), renal, hepatic,
hematological (including sickle cell disease), neurologic,
neuromuscular, or metabolic disorders (including diabetes mellitus);
- Immunosuppression, including that
caused by medications or by HIV;
- Pregnant women;
- Persons younger than 19 years of
age who are receiving long-term aspirin therapy;
- Residents of nursing homes and
other chronic-care facilities.
See:
http://www.cdc.gov/h1n1flu/recommendations.htm
Patients who contract the H1N1 virus
infection, but who are not in a high-risk group have had a self-limited
respiratory illness similar to typical seasonal influenza. For most of these
patients, the benefits of using antivirals may be modest. (Studies show it
only shortens the illness by approxamately 1 day). Therefore, testing,
treatment and chemoprophylaxis efforts should be directed primarily at
persons who are hospitalized or at higher risk for influenza complications.
Post exposure antiviral
chemoprophylaxis (giving medication to prevent illness when exposed) with
either oseltamivir or zanamivir can be considered for the following:
1. Close contacts of cases (confirmed,
probable, or suspected) who are at high-risk for complications of influenza
2. Health care personnel, public
health workers, or first responders who have had a recognized, unprotected
close contact exposure to a person with novel (H1N1) influenza virus
infection (confirmed, probable, or suspected) during that person’s
infectious period.
Interesting graphs:
Realize most adults will not go in and get tested but
will bring in their children. That is why there are
high numbers of kids.
As you can see there were a lot more cases in 07-08
year.
More in 07-08
This is scary but remember most (but not all) of these
are kids with other health issues.
This is out millions of children. You can see the second peak of cases
this summer.
